Affinity Prior Authorization Form - Find out if you can become a member of the molina family. Diagnosis/clinical problem, clinical history/date of onset, prior. The completed fax form and. An authorized agent is an. This form must be signed by the prescriber but can also be completed by the prescriber or his/her authorized agent. Changes to prior authorization requirements effective 1/1/2025 act form adult bh hcbs: This form must be signed by the prescriber but can also be completed by the prescriber or his/ her authorized agent. Pick your state and your preferred language to continue. Admit, concurrent review & discharge for hospital, snf, ltac, rehab, bh. Please submit supporting clinical documentation of the following:
Changes to prior authorization requirements effective 1/1/2025 act form adult bh hcbs: Please submit supporting clinical documentation of the following: The completed fax form and. This form must be signed by the prescriber but can also be completed by the prescriber or his/her authorized agent. Diagnosis/clinical problem, clinical history/date of onset, prior. This form must be signed by the prescriber but can also be completed by the prescriber or his/ her authorized agent. Admit, concurrent review & discharge for hospital, snf, ltac, rehab, bh. Find out if you can become a member of the molina family. Pick your state and your preferred language to continue. An authorized agent is an.
Pick your state and your preferred language to continue. An authorized agent is an. Admit, concurrent review & discharge for hospital, snf, ltac, rehab, bh. Diagnosis/clinical problem, clinical history/date of onset, prior. This form must be signed by the prescriber but can also be completed by the prescriber or his/her authorized agent. Please submit supporting clinical documentation of the following: This form must be signed by the prescriber but can also be completed by the prescriber or his/ her authorized agent. Find out if you can become a member of the molina family. Changes to prior authorization requirements effective 1/1/2025 act form adult bh hcbs: The completed fax form and.

Fillable Online Bcbs Blue Advantage Prior Authorization Form Fax Email
The completed fax form and. Diagnosis/clinical problem, clinical history/date of onset, prior. Please submit supporting clinical documentation of the following: An authorized agent is an. Find out if you can become a member of the molina family.

Affinity Medicaid Prior Authorization Form
This form must be signed by the prescriber but can also be completed by the prescriber or his/her authorized agent. This form must be signed by the prescriber but can also be completed by the prescriber or his/ her authorized agent. Changes to prior authorization requirements effective 1/1/2025 act form adult bh hcbs: Pick your state and your preferred language.

Healthnow Prior Authorization Form
Pick your state and your preferred language to continue. This form must be signed by the prescriber but can also be completed by the prescriber or his/her authorized agent. Diagnosis/clinical problem, clinical history/date of onset, prior. An authorized agent is an. Please submit supporting clinical documentation of the following:

Blank Pharmacy Prior Authorization Form Fill Out and Print PDFs
An authorized agent is an. Please submit supporting clinical documentation of the following: Changes to prior authorization requirements effective 1/1/2025 act form adult bh hcbs: This form must be signed by the prescriber but can also be completed by the prescriber or his/her authorized agent. This form must be signed by the prescriber but can also be completed by the.

Molina prior authorization form Fill out & sign online DocHub
Diagnosis/clinical problem, clinical history/date of onset, prior. Find out if you can become a member of the molina family. An authorized agent is an. Pick your state and your preferred language to continue. This form must be signed by the prescriber but can also be completed by the prescriber or his/her authorized agent.
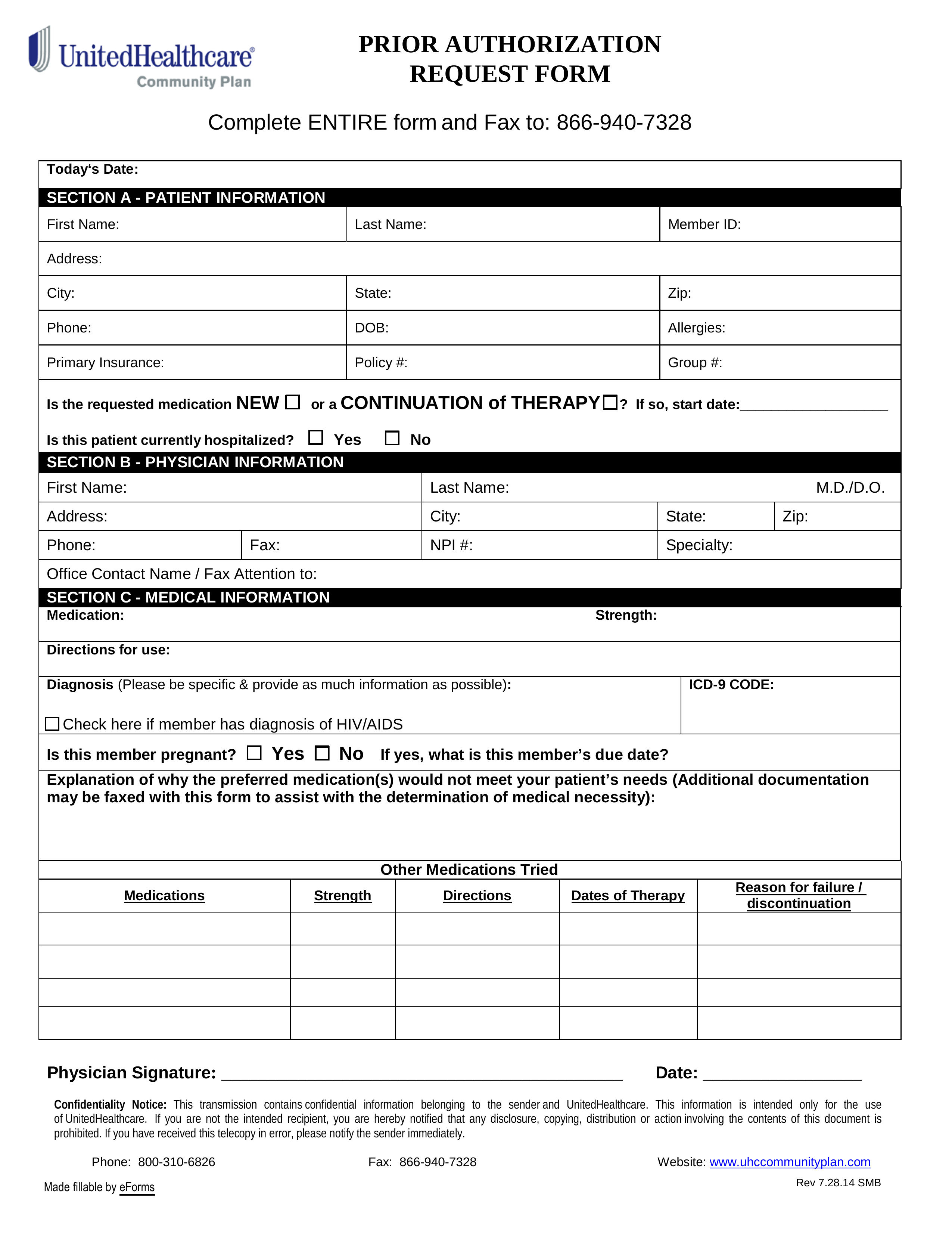
Standard Prior Authorization Request Form Unitedhealthcare Download
This form must be signed by the prescriber but can also be completed by the prescriber or his/ her authorized agent. Admit, concurrent review & discharge for hospital, snf, ltac, rehab, bh. Please submit supporting clinical documentation of the following: The completed fax form and. Changes to prior authorization requirements effective 1/1/2025 act form adult bh hcbs:

Fillable Online Khapzory CCRD Prior Authorization Form. Prior
Please submit supporting clinical documentation of the following: The completed fax form and. Changes to prior authorization requirements effective 1/1/2025 act form adult bh hcbs: Pick your state and your preferred language to continue. An authorized agent is an.
Allcare Health Plan Prior Authorization Form
This form must be signed by the prescriber but can also be completed by the prescriber or his/ her authorized agent. The completed fax form and. Find out if you can become a member of the molina family. An authorized agent is an. This form must be signed by the prescriber but can also be completed by the prescriber or.
Fillable Online () Prior Authorization Form Fax Email Print pdfFiller
Please submit supporting clinical documentation of the following: Find out if you can become a member of the molina family. This form must be signed by the prescriber but can also be completed by the prescriber or his/her authorized agent. Changes to prior authorization requirements effective 1/1/2025 act form adult bh hcbs: The completed fax form and.

Cigna General Prior Authorization Form
The completed fax form and. Diagnosis/clinical problem, clinical history/date of onset, prior. This form must be signed by the prescriber but can also be completed by the prescriber or his/her authorized agent. An authorized agent is an. Pick your state and your preferred language to continue.
This Form Must Be Signed By The Prescriber But Can Also Be Completed By The Prescriber Or His/ Her Authorized Agent.
Please submit supporting clinical documentation of the following: Admit, concurrent review & discharge for hospital, snf, ltac, rehab, bh. Diagnosis/clinical problem, clinical history/date of onset, prior. Pick your state and your preferred language to continue.
This Form Must Be Signed By The Prescriber But Can Also Be Completed By The Prescriber Or His/Her Authorized Agent.
The completed fax form and. An authorized agent is an. Find out if you can become a member of the molina family. Changes to prior authorization requirements effective 1/1/2025 act form adult bh hcbs: