De 1000A Appeal Form - How can i file an appeal? Many of our forms and publications are available online and can be easily downloaded and printed by following the links below. As shown on the enclosed notice of determination, you are not eligible for all or part of the period claimed. To appeal this decision to an. In the form, explain why you do not agree with the. Complete the appeal form (de 1000a) electronically or by mail. Please be sure to include your social security. Complete the enclosed appeal form, de 1000a, or write a letter stating that you want to appeal. To appeal a decision, complete the appeal form (de 1000a) and submit it within 30 days. If we are not able to pay your disability insurance (di) or paid family leave (pfl) benefits, we will send you an appeal form (de 1000a) with your.
For example, the state of california requires you to complete appeal form de 1000a if you are disqualified from receiving benefits. How can i file an appeal? In the form, explain why you do not agree with the. Complete the enclosed appeal form, de 1000a, or write a letter stating that you want to appeal. To appeal this decision to an. Many of our forms and publications are available online and can be easily downloaded and printed by following the links below. If we are not able to pay your disability insurance (di) or paid family leave (pfl) benefits, we will send you an appeal form (de 1000a) with your. Please be sure to include your social security. To appeal a decision, complete the appeal form (de 1000a) and submit it within 30 days. As shown on the enclosed notice of determination, you are not eligible for all or part of the period claimed.
Complete the enclosed appeal form, de 1000a, or write a letter stating that you want to appeal. If we are not able to pay your disability insurance (di) or paid family leave (pfl) benefits, we will send you an appeal form (de 1000a) with your. To appeal this decision to an. As shown on the enclosed notice of determination, you are not eligible for all or part of the period claimed. Complete the appeal form (de 1000a) electronically or by mail. Please be sure to include your social security. For example, the state of california requires you to complete appeal form de 1000a if you are disqualified from receiving benefits. Many of our forms and publications are available online and can be easily downloaded and printed by following the links below. In the form, explain why you do not agree with the. To appeal a decision, complete the appeal form (de 1000a) and submit it within 30 days.
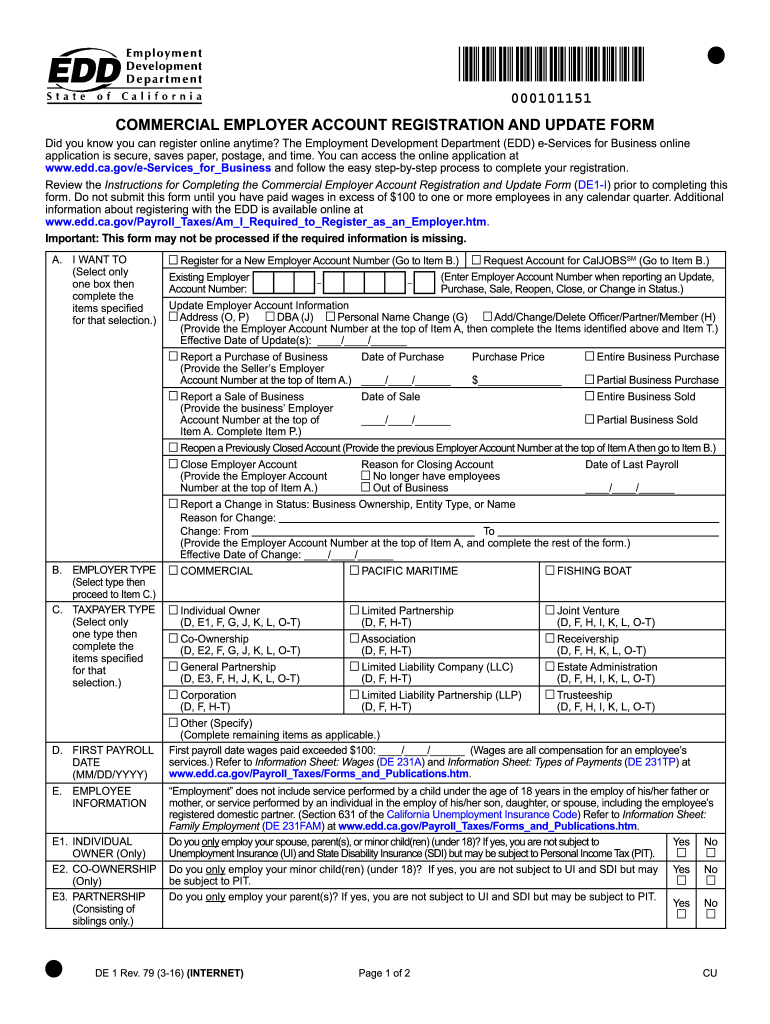
20162024 Form CA DE 1 Fill Online, Printable, Fillable, Blank pdfFiller
For example, the state of california requires you to complete appeal form de 1000a if you are disqualified from receiving benefits. Please be sure to include your social security. Many of our forms and publications are available online and can be easily downloaded and printed by following the links below. To appeal a decision, complete the appeal form (de 1000a).

Termination Appeal Letter Forms Docs 2023
Complete the enclosed appeal form, de 1000a, or write a letter stating that you want to appeal. Many of our forms and publications are available online and can be easily downloaded and printed by following the links below. For example, the state of california requires you to complete appeal form de 1000a if you are disqualified from receiving benefits. Please.
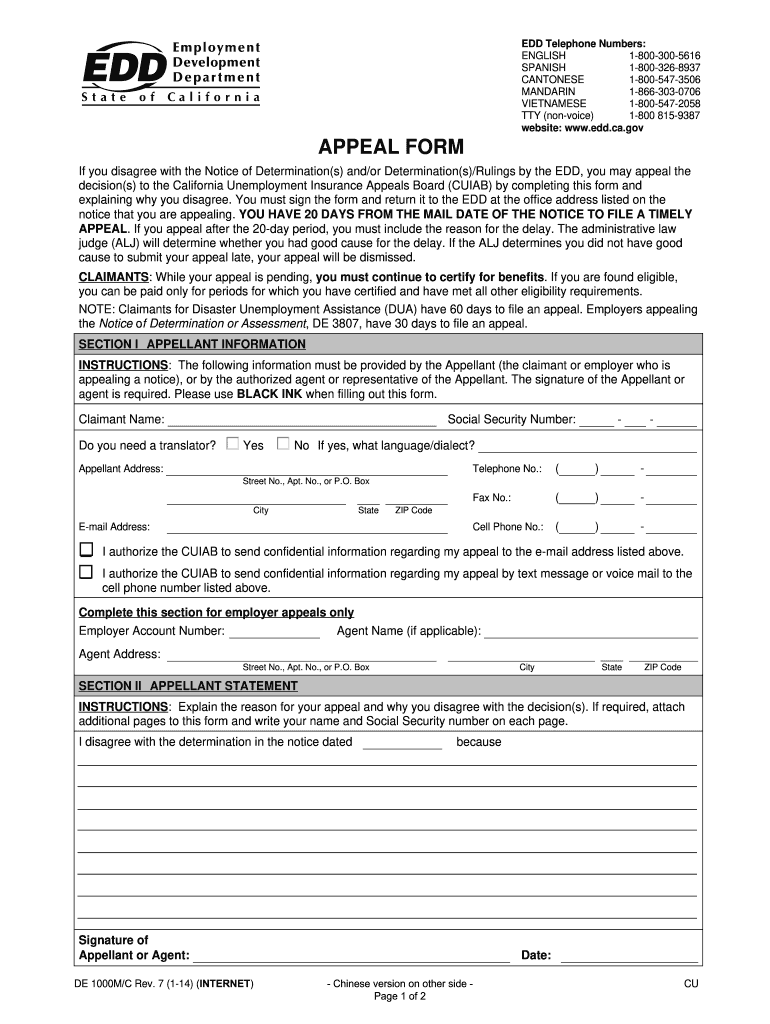
20142025 Form CA EDD DE 1000M/C Fill Online, Printable, Fillable
For example, the state of california requires you to complete appeal form de 1000a if you are disqualified from receiving benefits. In the form, explain why you do not agree with the. If we are not able to pay your disability insurance (di) or paid family leave (pfl) benefits, we will send you an appeal form (de 1000a) with your..
Appeal Form (De 1000M/T) Edit, Fill, Sign Online Handypdf
As shown on the enclosed notice of determination, you are not eligible for all or part of the period claimed. How can i file an appeal? Please be sure to include your social security. To appeal this decision to an. In the form, explain why you do not agree with the.
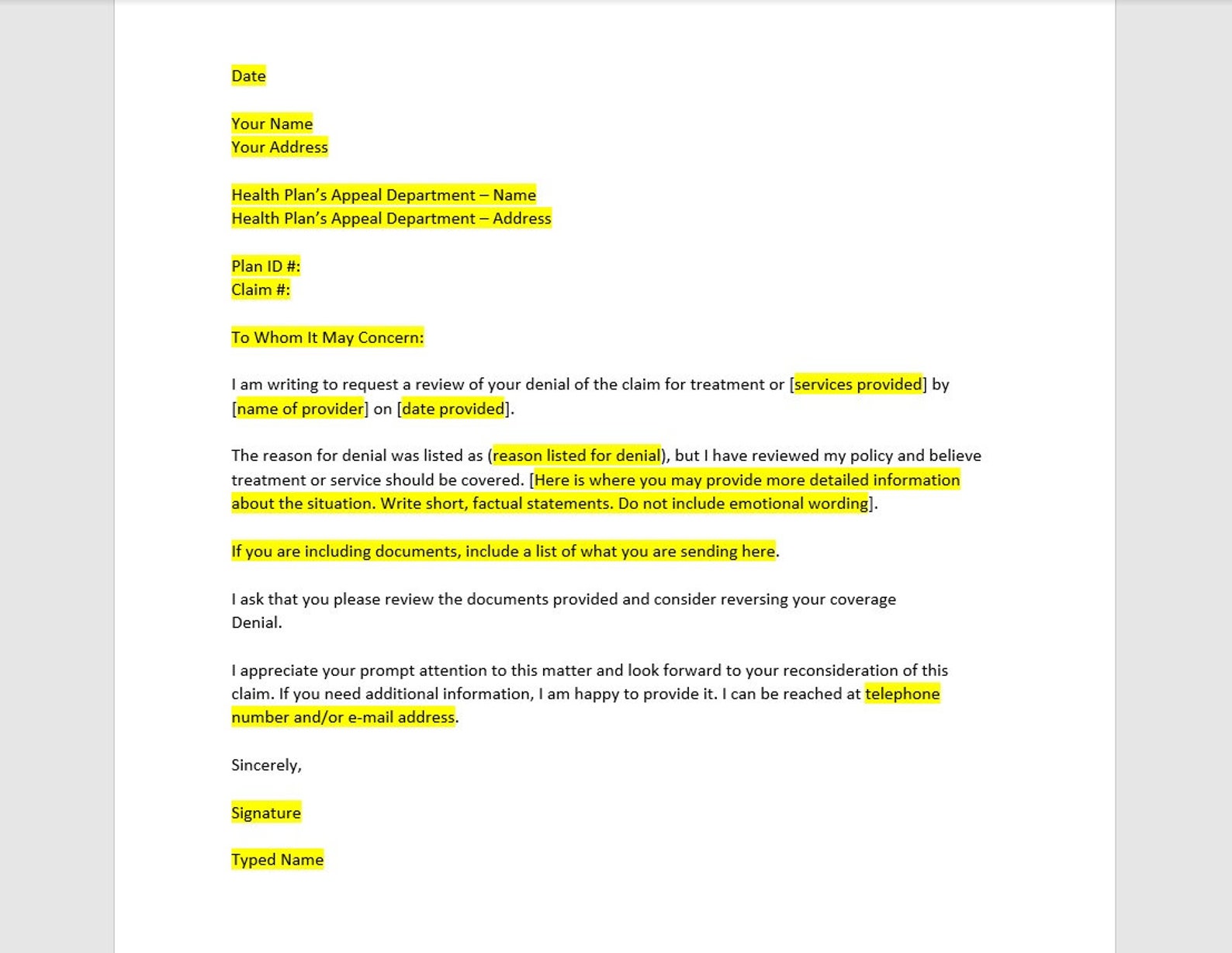
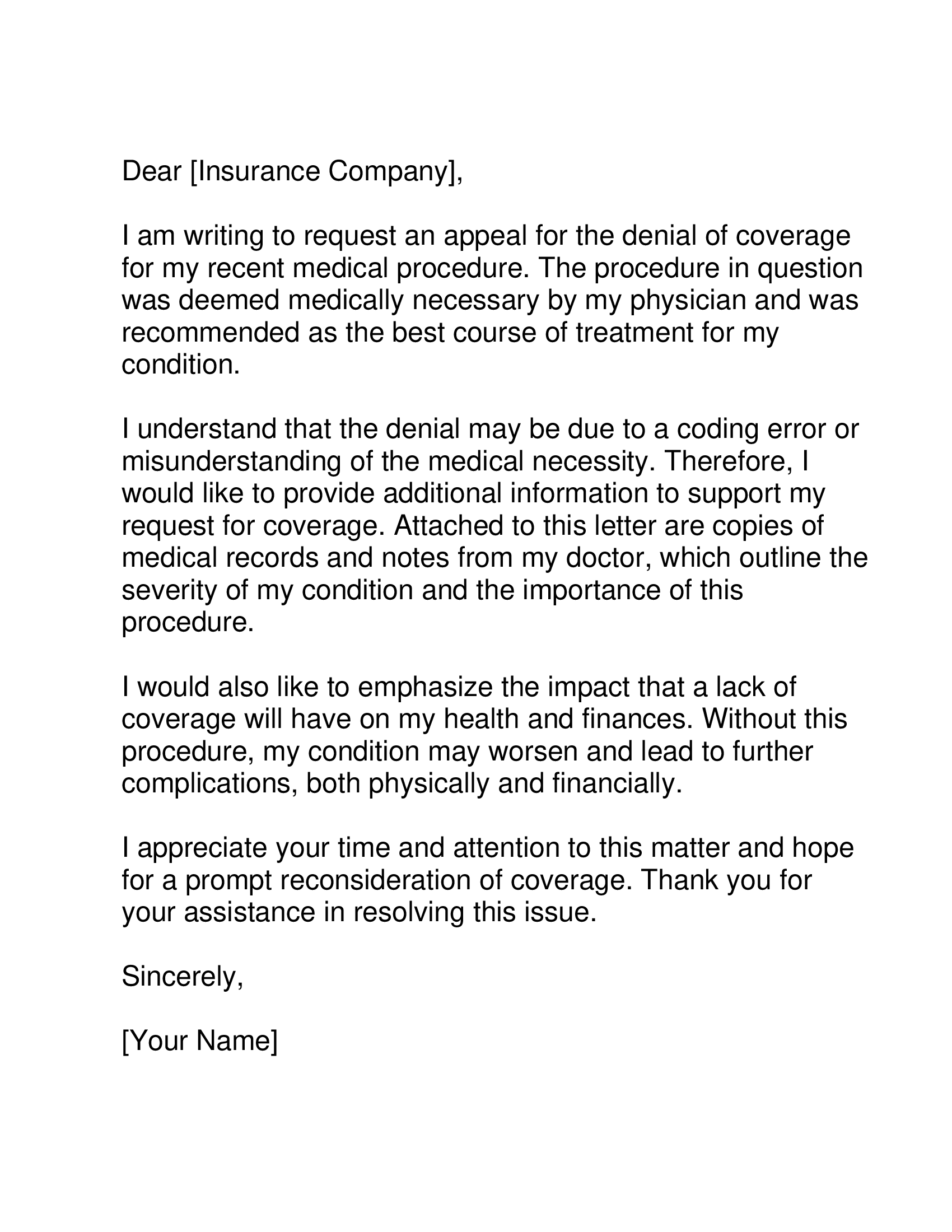
Health Insurance Appeal Letter Template, Health Insurance Appeal Letter
In the form, explain why you do not agree with the. Complete the enclosed appeal form, de 1000a, or write a letter stating that you want to appeal. For example, the state of california requires you to complete appeal form de 1000a if you are disqualified from receiving benefits. Many of our forms and publications are available online and can.

20192024 MA HCAS Universal Provider Request for Claim Review Form Fill
Please be sure to include your social security. To appeal this decision to an. For example, the state of california requires you to complete appeal form de 1000a if you are disqualified from receiving benefits. Complete the enclosed appeal form, de 1000a, or write a letter stating that you want to appeal. In the form, explain why you do not.
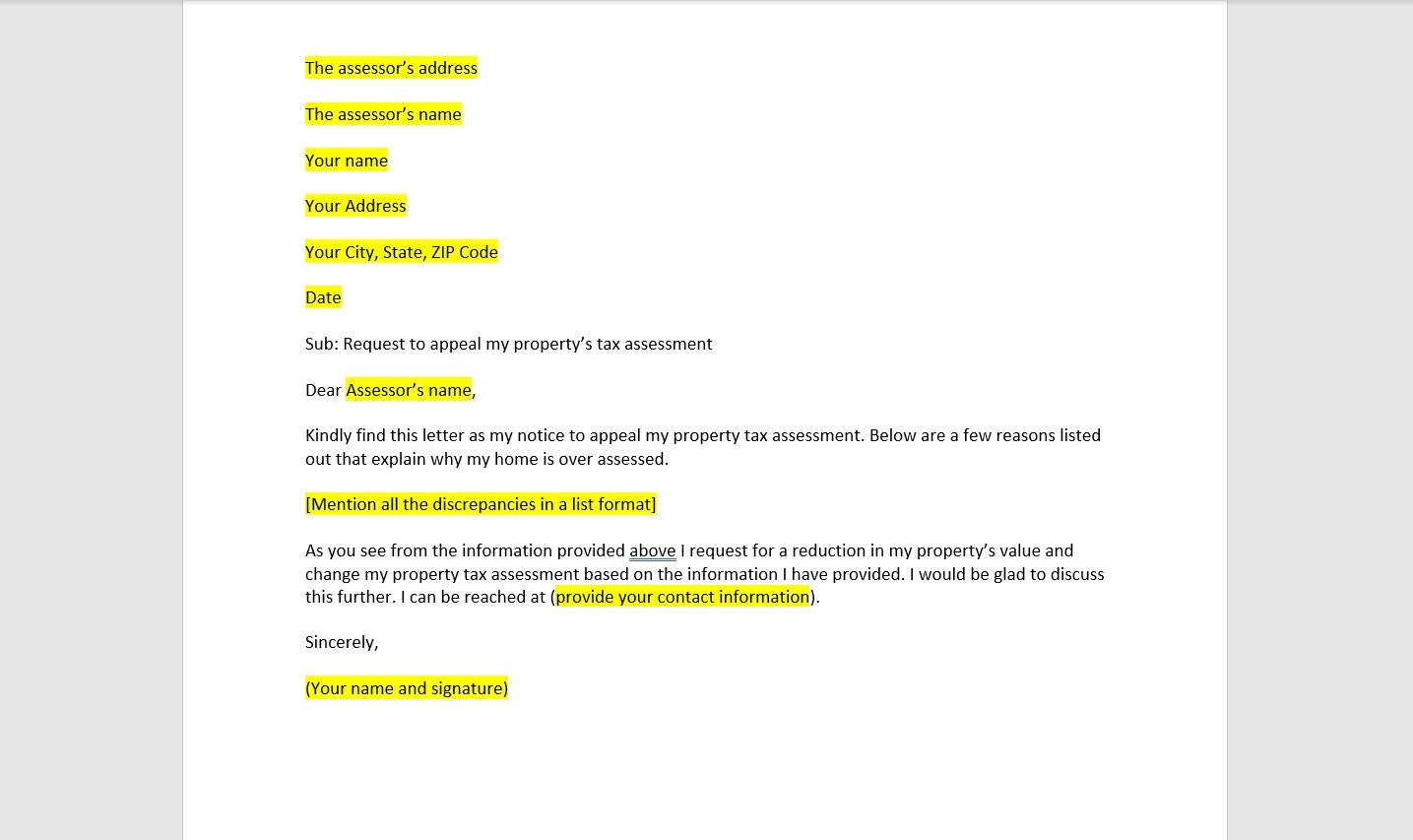
Property Tax Appeal Letter Template, Property Tax Appeal Letter
Complete the appeal form (de 1000a) electronically or by mail. As shown on the enclosed notice of determination, you are not eligible for all or part of the period claimed. Complete the enclosed appeal form, de 1000a, or write a letter stating that you want to appeal. In the form, explain why you do not agree with the. To appeal.

20162024 Form CA EDD DE 1000AA Fill Online, Printable, Fillable, Blank
Complete the appeal form (de 1000a) electronically or by mail. Please be sure to include your social security. As shown on the enclosed notice of determination, you are not eligible for all or part of the period claimed. In the form, explain why you do not agree with the. Many of our forms and publications are available online and can.
Medicare Irmaa 2024 Appeal Form Pdf Sella Daniella
Complete the appeal form (de 1000a) electronically or by mail. As shown on the enclosed notice of determination, you are not eligible for all or part of the period claimed. How can i file an appeal? In the form, explain why you do not agree with the. For example, the state of california requires you to complete appeal form de.
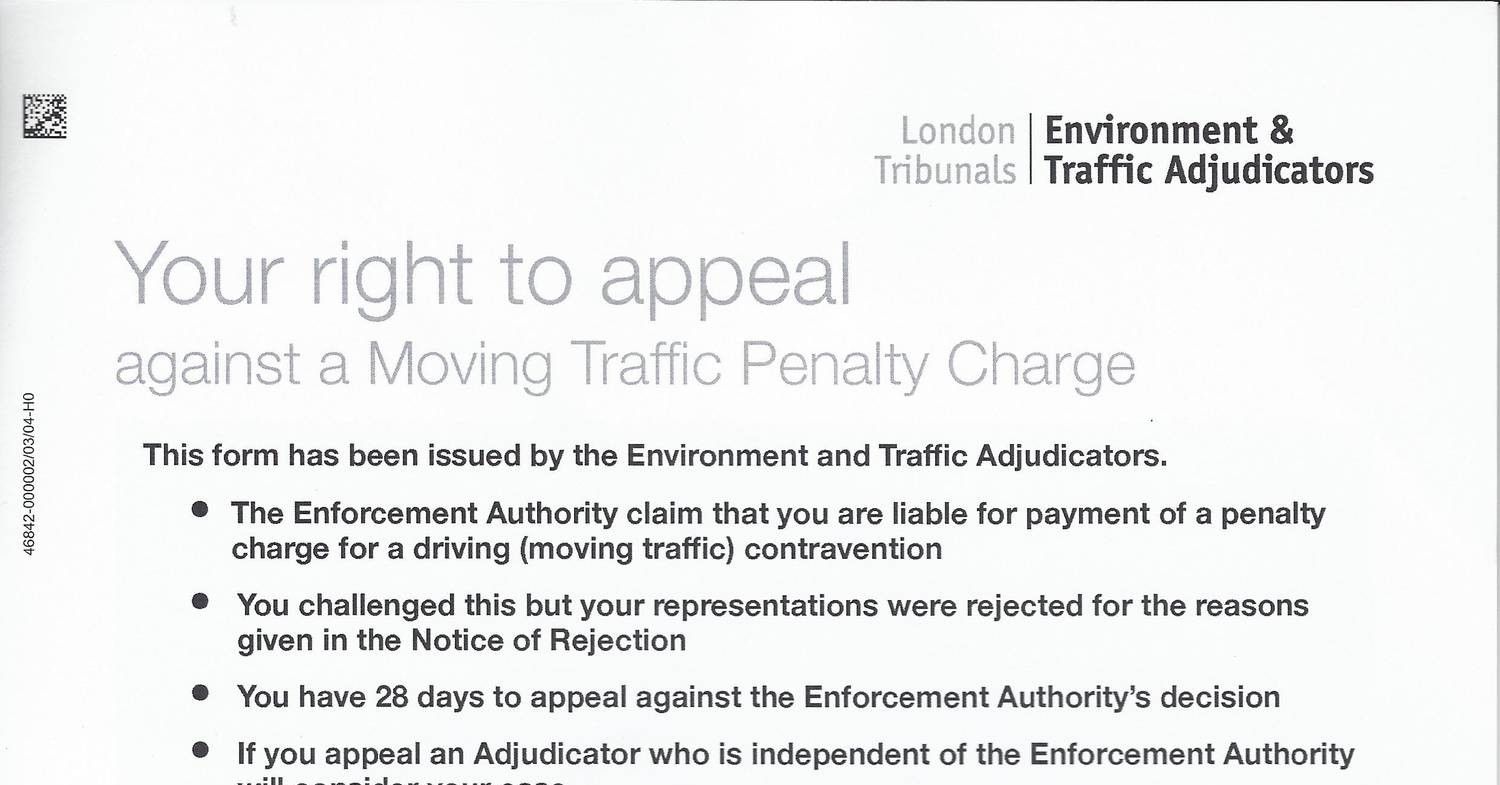
Right_to_Appeal_form.pdf DocDroid
In the form, explain why you do not agree with the. To appeal a decision, complete the appeal form (de 1000a) and submit it within 30 days. Complete the enclosed appeal form, de 1000a, or write a letter stating that you want to appeal. Please be sure to include your social security. As shown on the enclosed notice of determination,.
Complete The Enclosed Appeal Form, De 1000A, Or Write A Letter Stating That You Want To Appeal.
For example, the state of california requires you to complete appeal form de 1000a if you are disqualified from receiving benefits. To appeal a decision, complete the appeal form (de 1000a) and submit it within 30 days. In the form, explain why you do not agree with the. Complete the appeal form (de 1000a) electronically or by mail.
To Appeal This Decision To An.
As shown on the enclosed notice of determination, you are not eligible for all or part of the period claimed. If we are not able to pay your disability insurance (di) or paid family leave (pfl) benefits, we will send you an appeal form (de 1000a) with your. How can i file an appeal? Please be sure to include your social security.