Moda Appeal Form - Box 40384, portland, or 97204 or faxed to 503. Submit a written request and mail to: Request for reconsideration should be sent to moda health, attn: Medicare appeals unit at p.o. Box 40384, portland, or 97240 or fax to 503. Use this form to name a relative, friend, advocate, doctor or anyone else as your appointed representative. Medicare appeal and grievance unit p.o. Mail this form to moda health: Appointment of representative form : Mail this form to moda health:
Use this form to name a relative, friend, advocate, doctor or anyone else as your appointed representative. Box 40384, portland, or 97204 or faxed to 503. Complaint and appeal form ready to submit? Mail this form to moda health, attn: Box 40384, portland, or 97240 or fax to 503. Medicare appeal and grievance unit p.o. Appointment of representative form : Submit a written request and mail to: Medicare appeals unit at p.o. Mail this form to moda health:
Medicare appeals unit at p.o. Appointment of representative form : Box 40384, portland, or 97204 or faxed to 503. Use this form to name a relative, friend, advocate, doctor or anyone else as your appointed representative. Complaint and appeal form ready to submit? Mail this form to moda health, attn: Submit a written request and mail to: Mail this form to moda health: Medicare appeal and grievance unit p.o. Mail this form to moda health:
Fillable Online Appeal FormMeter Fax Email Print pdfFiller
Submit a written request and mail to: Appointment of representative form : Use this form to name a relative, friend, advocate, doctor or anyone else as your appointed representative. Complaint and appeal form ready to submit? Box 40384, portland, or 97204 or faxed to 503.
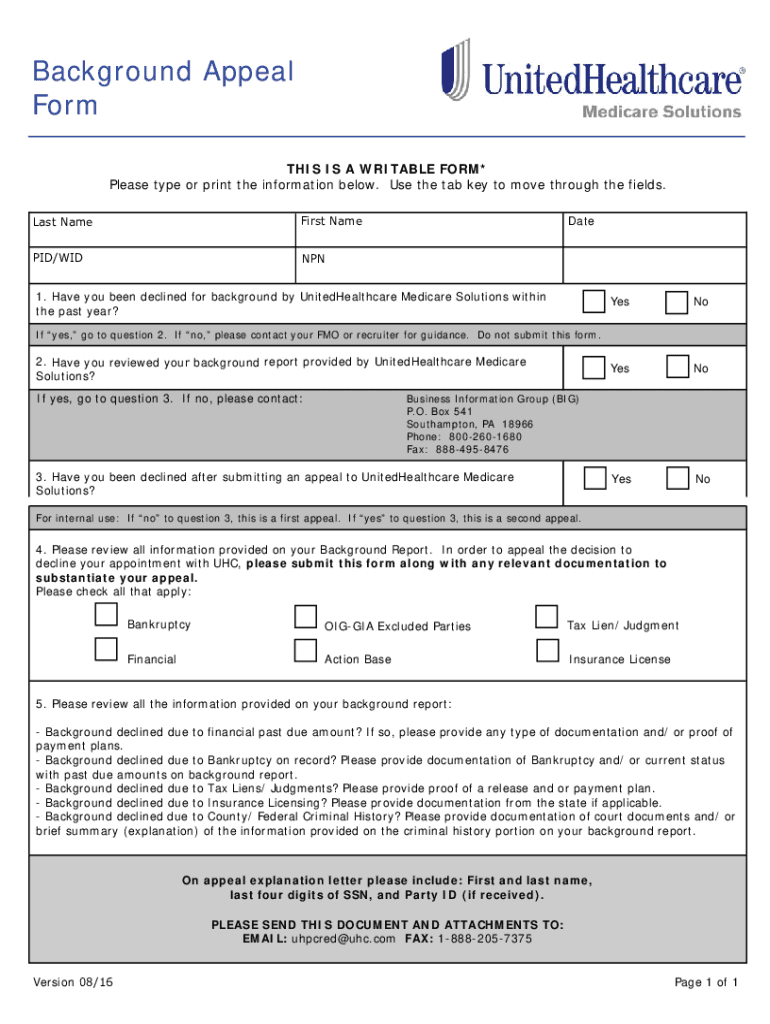
United Healthcare Provider Appeal 20162024 Form Fill Out and Sign
Complaint and appeal form ready to submit? Medicare appeals unit at p.o. Submit a written request and mail to: Appointment of representative form : Box 40384, portland, or 97240 or fax to 503.
College Appeal Letter Forms Docs 2023
Medicare appeal and grievance unit p.o. Request for reconsideration should be sent to moda health, attn: Medicare appeals unit at p.o. Submit a written request and mail to: Use this form to name a relative, friend, advocate, doctor or anyone else as your appointed representative.

FM BHS SUPT Appeal Form Arabic PDF
Mail this form to moda health: Submit a written request and mail to: Appointment of representative form : Request for reconsideration should be sent to moda health, attn: Medicare appeal and grievance unit p.o.
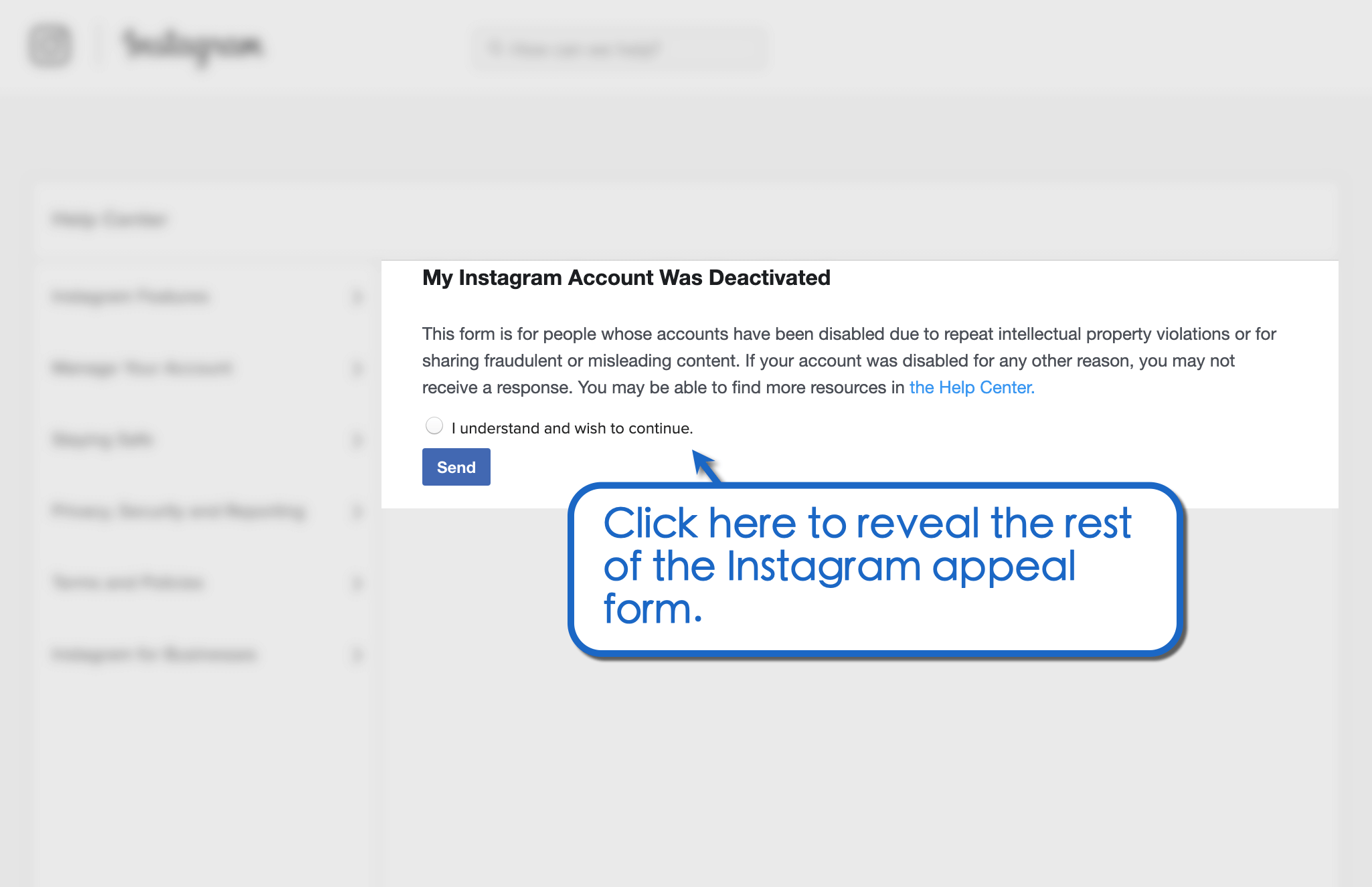
How to Use the Instagram Appeal Form for Banned Profiles Vista Social
Use this form to name a relative, friend, advocate, doctor or anyone else as your appointed representative. Complaint and appeal form ready to submit? Mail this form to moda health: Mail this form to moda health, attn: Box 40384, portland, or 97204 or faxed to 503.
Proposed Appeal Complete with ease airSlate SignNow
Mail this form to moda health: Complaint and appeal form ready to submit? Use this form to name a relative, friend, advocate, doctor or anyone else as your appointed representative. Appointment of representative form : Mail this form to moda health, attn:
Petition on Appeal Form Fill Out and Sign Printable PDF Template
Box 40384, portland, or 97204 or faxed to 503. Mail this form to moda health, attn: Mail this form to moda health: Medicare appeals unit at p.o. Medicare appeal and grievance unit p.o.
Professional Medical Appeal Form Template PDF Minasinternational
Use this form to name a relative, friend, advocate, doctor or anyone else as your appointed representative. Mail this form to moda health, attn: Request for reconsideration should be sent to moda health, attn: Mail this form to moda health: Medicare appeal and grievance unit p.o.
Ssa44 Form 2024 Irmaa Appeal Form 2024 Online Tori Jeannine
Mail this form to moda health: Box 40384, portland, or 97240 or fax to 503. Use this form to name a relative, friend, advocate, doctor or anyone else as your appointed representative. Request for reconsideration should be sent to moda health, attn: Appointment of representative form :
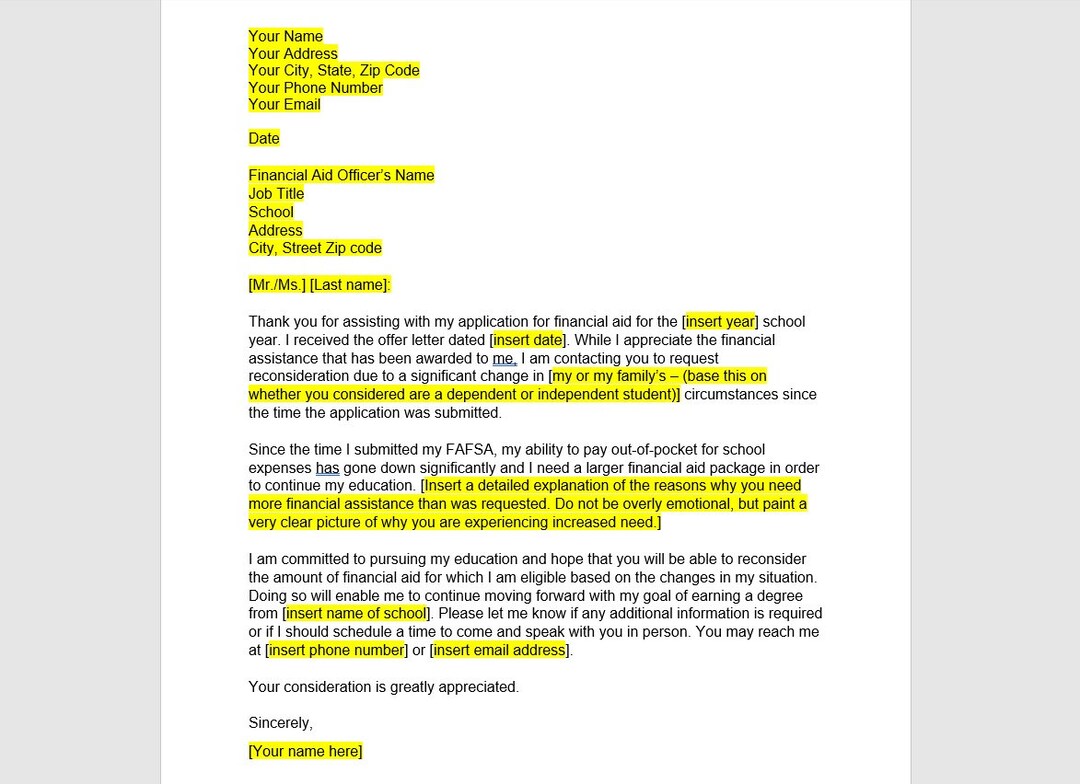
Financial Aid Appeal Letter Template, Financial Aid Appeal Letter
Use this form to name a relative, friend, advocate, doctor or anyone else as your appointed representative. Mail this form to moda health: Mail this form to moda health, attn: Box 40384, portland, or 97240 or fax to 503. Appointment of representative form :
Mail This Form To Moda Health:
Appointment of representative form : Submit a written request and mail to: Medicare appeals unit at p.o. Request for reconsideration should be sent to moda health, attn:
Use This Form To Name A Relative, Friend, Advocate, Doctor Or Anyone Else As Your Appointed Representative.
Box 40384, portland, or 97240 or fax to 503. Mail this form to moda health: Medicare appeal and grievance unit p.o. Mail this form to moda health, attn:
Box 40384, Portland, Or 97204 Or Faxed To 503.
Complaint and appeal form ready to submit?