Patient Chief Complaint Form - ______________________________________________________________________________ did your problem result from a specific injury? As our patient we want you to know that we respect the privacy of your. _____ _____ _____ _____ first mi last preferred name Why are you here today? Are you now or have you been within the past two years under any other doctor’s care for any reason? Please complete the following section only if your chief complaint/symptoms were due to an accident or injury. Patient to carry out treatment, payment, or health care operations. By signing this form, i permit baptist medical group (bmg) staff to discuss information about me with the people listed below. If you feel that your symptoms are an emergency, you should seek immediate medical attention at the nearest emergency room.
Patient to carry out treatment, payment, or health care operations. Please complete the following section only if your chief complaint/symptoms were due to an accident or injury. As our patient we want you to know that we respect the privacy of your. _____ _____ _____ _____ first mi last preferred name ______________________________________________________________________________ did your problem result from a specific injury? Are you now or have you been within the past two years under any other doctor’s care for any reason? Why are you here today? By signing this form, i permit baptist medical group (bmg) staff to discuss information about me with the people listed below. If you feel that your symptoms are an emergency, you should seek immediate medical attention at the nearest emergency room.
_____ _____ _____ _____ first mi last preferred name If you feel that your symptoms are an emergency, you should seek immediate medical attention at the nearest emergency room. Why are you here today? Patient to carry out treatment, payment, or health care operations. Please complete the following section only if your chief complaint/symptoms were due to an accident or injury. By signing this form, i permit baptist medical group (bmg) staff to discuss information about me with the people listed below. Are you now or have you been within the past two years under any other doctor’s care for any reason? As our patient we want you to know that we respect the privacy of your. ______________________________________________________________________________ did your problem result from a specific injury?
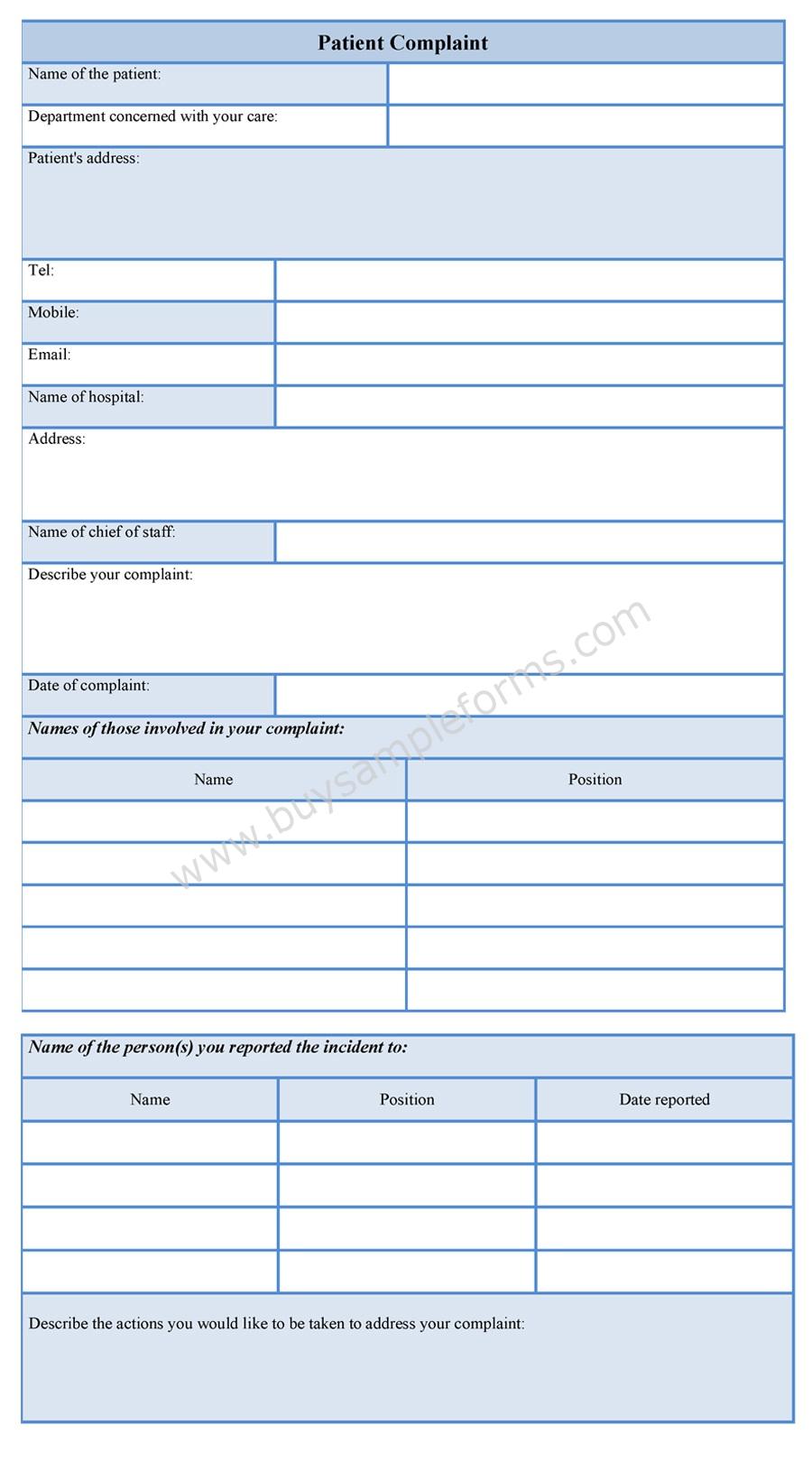
Patient Complaint Form
_____ _____ _____ _____ first mi last preferred name If you feel that your symptoms are an emergency, you should seek immediate medical attention at the nearest emergency room. As our patient we want you to know that we respect the privacy of your. Patient to carry out treatment, payment, or health care operations. Are you now or have you.
FREE 11+ Sample Patient Complaint Forms in PDF Word
Please complete the following section only if your chief complaint/symptoms were due to an accident or injury. Why are you here today? If you feel that your symptoms are an emergency, you should seek immediate medical attention at the nearest emergency room. As our patient we want you to know that we respect the privacy of your. ______________________________________________________________________________ did your.

Chief Complaint Runny Nose. Paper Patient Health History Form Stock
______________________________________________________________________________ did your problem result from a specific injury? By signing this form, i permit baptist medical group (bmg) staff to discuss information about me with the people listed below. Why are you here today? Please complete the following section only if your chief complaint/symptoms were due to an accident or injury. Are you now or have you been within.
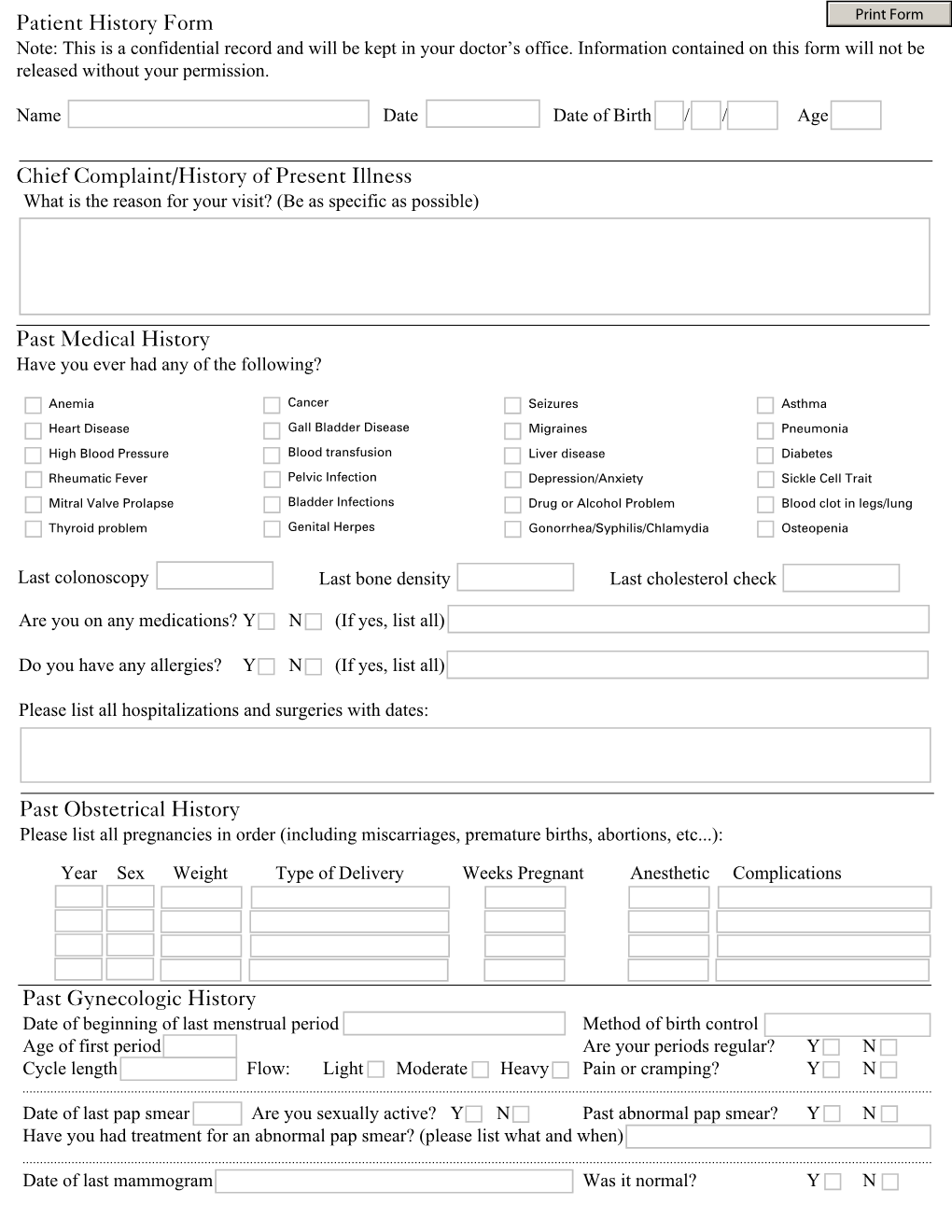
Patient History Form Chief Complaint/History of Present Illness DocsLib
Patient to carry out treatment, payment, or health care operations. Please complete the following section only if your chief complaint/symptoms were due to an accident or injury. _____ _____ _____ _____ first mi last preferred name Are you now or have you been within the past two years under any other doctor’s care for any reason? ______________________________________________________________________________ did your problem.
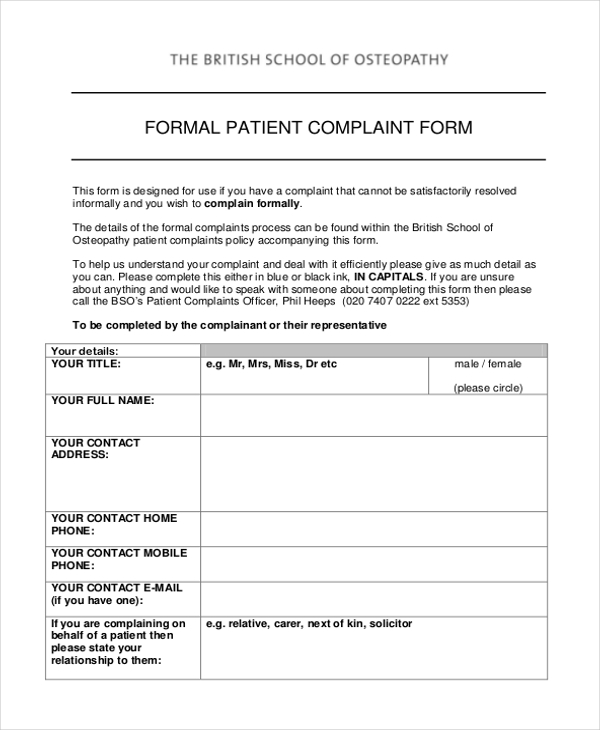
FREE 8+ Patient Complaint Forms in PDF MS Word
Please complete the following section only if your chief complaint/symptoms were due to an accident or injury. By signing this form, i permit baptist medical group (bmg) staff to discuss information about me with the people listed below. Patient to carry out treatment, payment, or health care operations. As our patient we want you to know that we respect the.
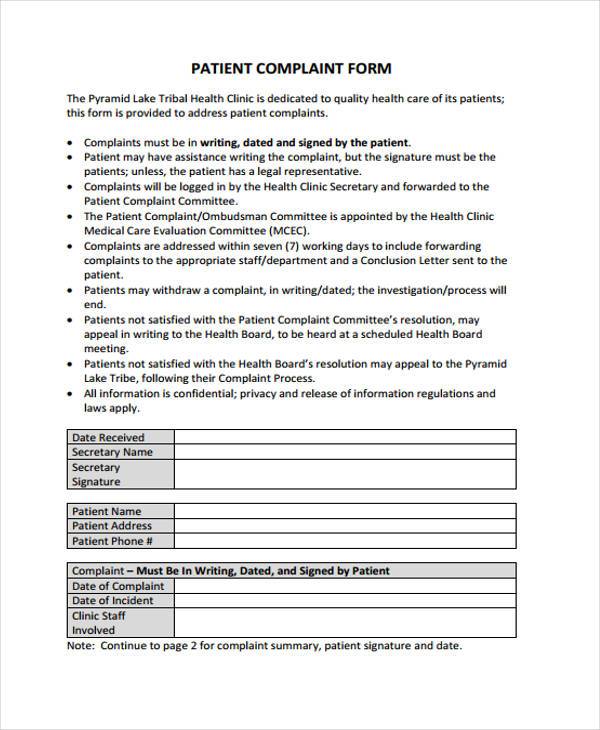
FREE 11+ Sample Patient Complaint Forms in PDF Word
If you feel that your symptoms are an emergency, you should seek immediate medical attention at the nearest emergency room. ______________________________________________________________________________ did your problem result from a specific injury? Are you now or have you been within the past two years under any other doctor’s care for any reason? Please complete the following section only if your chief complaint/symptoms were.

Patient Complaint Fillable PDF Form Editable PDF Forms
Patient to carry out treatment, payment, or health care operations. Why are you here today? Please complete the following section only if your chief complaint/symptoms were due to an accident or injury. By signing this form, i permit baptist medical group (bmg) staff to discuss information about me with the people listed below. Are you now or have you been.

Chief Complaint Form PDF Headache Symptoms And Signs
As our patient we want you to know that we respect the privacy of your. Why are you here today? Patient to carry out treatment, payment, or health care operations. ______________________________________________________________________________ did your problem result from a specific injury? By signing this form, i permit baptist medical group (bmg) staff to discuss information about me with the people listed below.
FREE 11+ Sample Patient Complaint Forms in PDF Word
Please complete the following section only if your chief complaint/symptoms were due to an accident or injury. _____ _____ _____ _____ first mi last preferred name Are you now or have you been within the past two years under any other doctor’s care for any reason? If you feel that your symptoms are an emergency, you should seek immediate medical.
FREE 8+ Patient Complaint Forms in PDF MS Word
Are you now or have you been within the past two years under any other doctor’s care for any reason? Please complete the following section only if your chief complaint/symptoms were due to an accident or injury. Patient to carry out treatment, payment, or health care operations. _____ _____ _____ _____ first mi last preferred name As our patient we.
______________________________________________________________________________ Did Your Problem Result From A Specific Injury?
_____ _____ _____ _____ first mi last preferred name Are you now or have you been within the past two years under any other doctor’s care for any reason? By signing this form, i permit baptist medical group (bmg) staff to discuss information about me with the people listed below. As our patient we want you to know that we respect the privacy of your.
Why Are You Here Today?
Please complete the following section only if your chief complaint/symptoms were due to an accident or injury. If you feel that your symptoms are an emergency, you should seek immediate medical attention at the nearest emergency room. Patient to carry out treatment, payment, or health care operations.