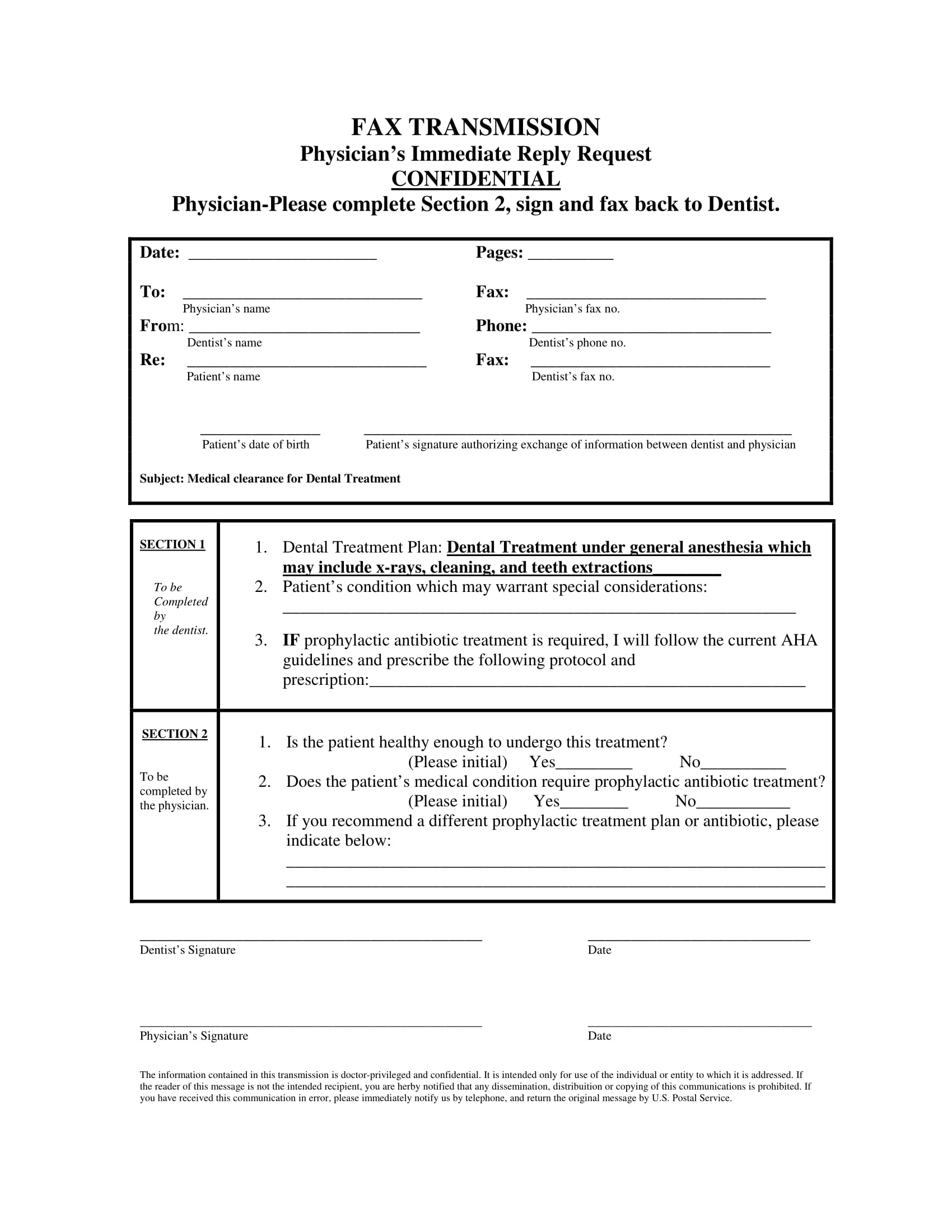
Printableprintable Medical Clearance Form For Dental Treatment - Medical clearance for dental treatment date: We appreciate your assistance in providing optimum care for this patient. Our mutual patient has presented for dental treatment with the following medical problem(s): This form is essential for obtaining medical clearance prior to dental treatment. Medical clearance for dental treatment form. It ensures that the patient's medical history is reviewed by a. The following treatment is scheduled in our. In an attempt to provide the best and safest dental care for this patient, we are requesting medical consultation and authorization. This document is essential for obtaining medical clearance prior to dental procedures. Our mutual patient is scheduled for dental treatment.
The following treatment is scheduled in our. It ensures that the patient's medical history is reviewed by a. Medical clearance for dental treatment form. Our mutual patient, as noted above, is scheduled for. Medical clearance for dental treatment date: Our mutual patient has presented for dental treatment with the following medical problem(s): In an attempt to provide the best and safest dental care for this patient, we are requesting medical consultation and authorization. This document is essential for obtaining medical clearance prior to dental procedures. This form is essential for obtaining medical clearance prior to dental treatment. Our mutual patient is scheduled for dental treatment.
This form is essential for obtaining medical clearance prior to dental treatment. Medical clearance for dental treatment date: Medical clearance for dental treatment form. Our mutual patient is scheduled for dental treatment. It ensures that the patient's medical history is reviewed by a. Our mutual patient has presented for dental treatment with the following medical problem(s): In an attempt to provide the best and safest dental care for this patient, we are requesting medical consultation and authorization. This document is essential for obtaining medical clearance prior to dental procedures. The following treatment is scheduled in our. We appreciate your assistance in providing optimum care for this patient.

Printable Medical Clearance Form For Dental Treatment
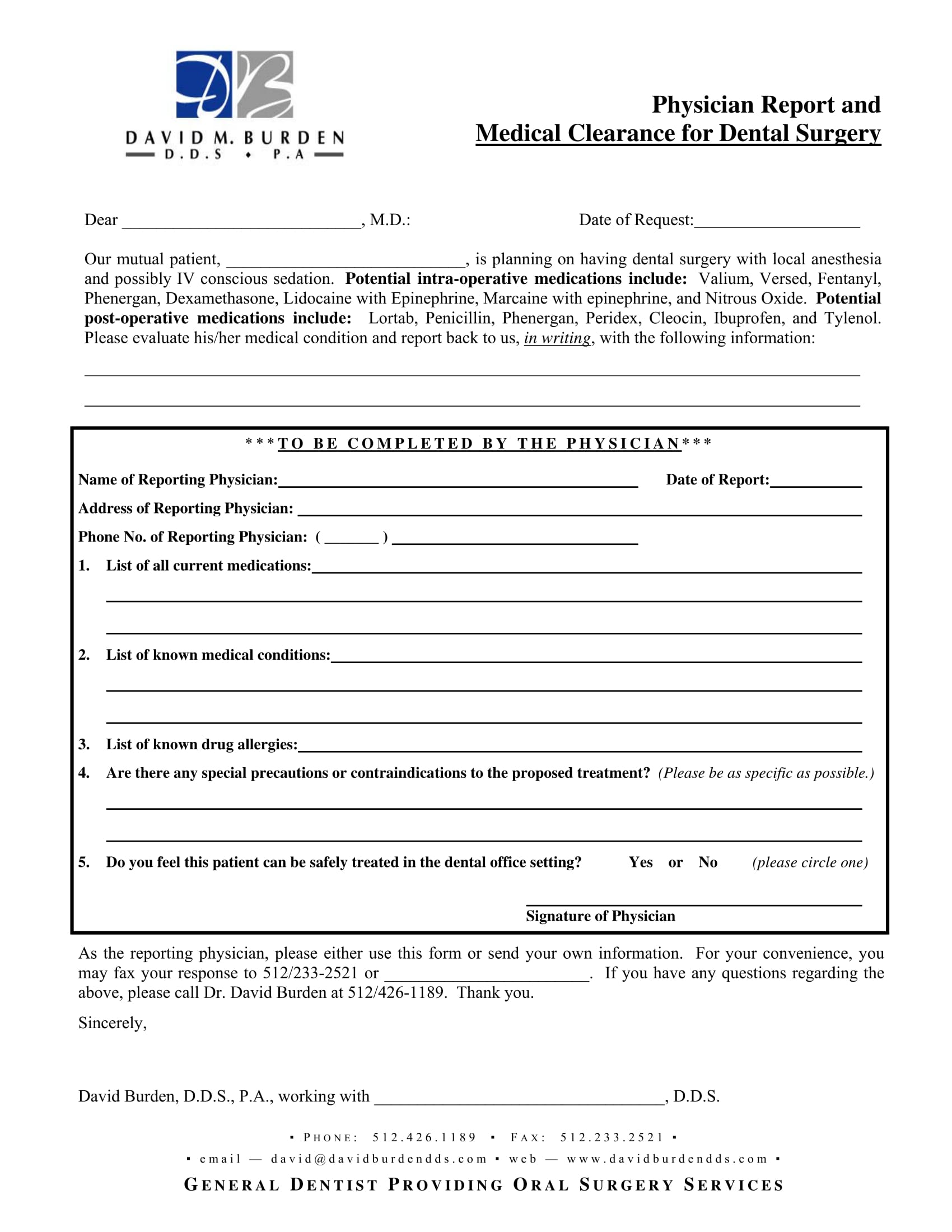
Our mutual patient is scheduled for dental treatment. Our mutual patient has presented for dental treatment with the following medical problem(s): Medical clearance for dental treatment date: In an attempt to provide the best and safest dental care for this patient, we are requesting medical consultation and authorization. This document is essential for obtaining medical clearance prior to dental procedures.
Printable Medical Clearance Form For Dental Treatment Printable Word
In an attempt to provide the best and safest dental care for this patient, we are requesting medical consultation and authorization. Our mutual patient has presented for dental treatment with the following medical problem(s): Medical clearance for dental treatment date: The following treatment is scheduled in our. This form is essential for obtaining medical clearance prior to dental treatment.
Printable Medical Clearance Form For Surgery Printable Forms Free Online
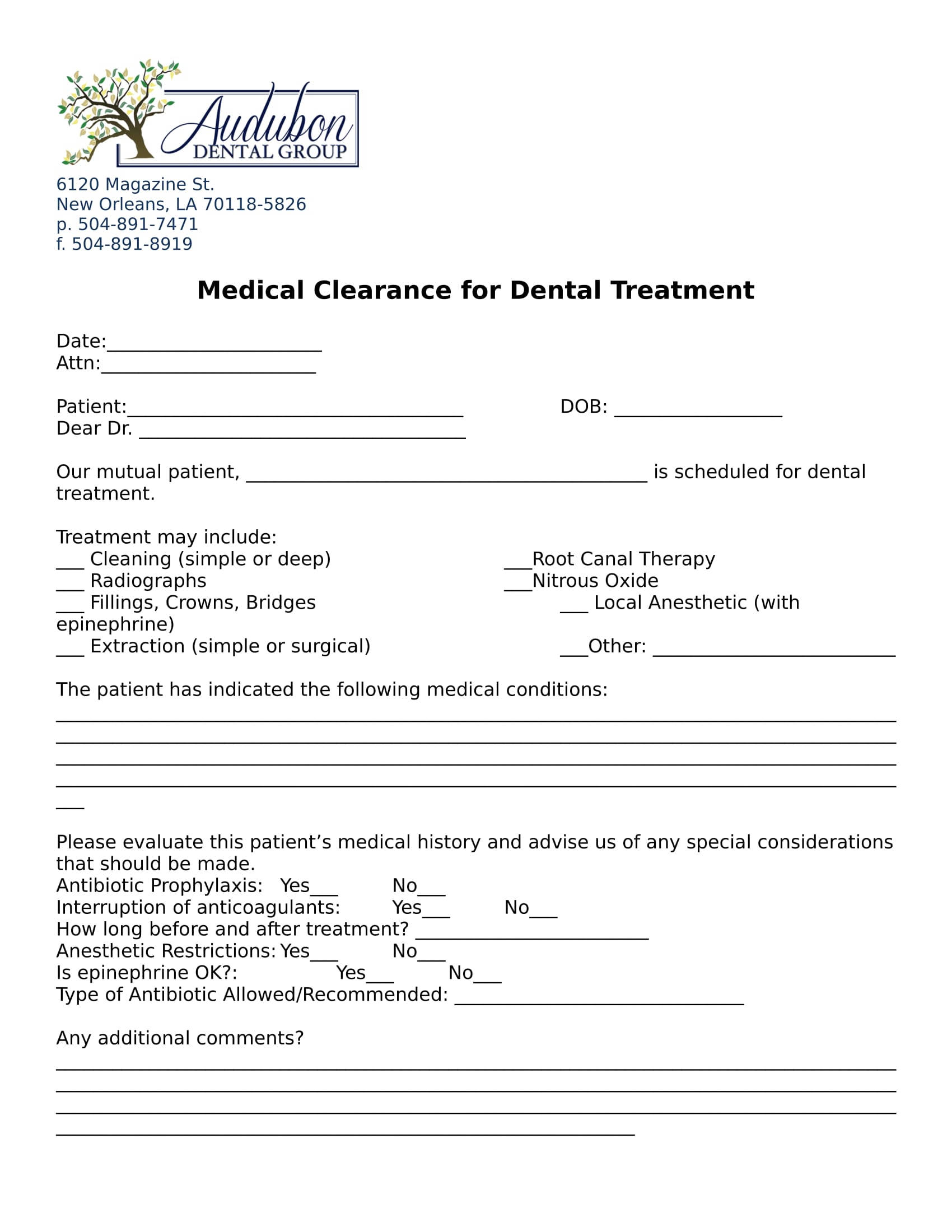
Medical clearance for dental treatment date: Our mutual patient has presented for dental treatment with the following medical problem(s): Medical clearance for dental treatment form. Our mutual patient, as noted above, is scheduled for. It ensures that the patient's medical history is reviewed by a.
Printable Medical Clearance Form For Dental Treatment Printable Forms
Medical clearance for dental treatment form. The following treatment is scheduled in our. Medical clearance for dental treatment date: Our mutual patient, as noted above, is scheduled for. Our mutual patient is scheduled for dental treatment.

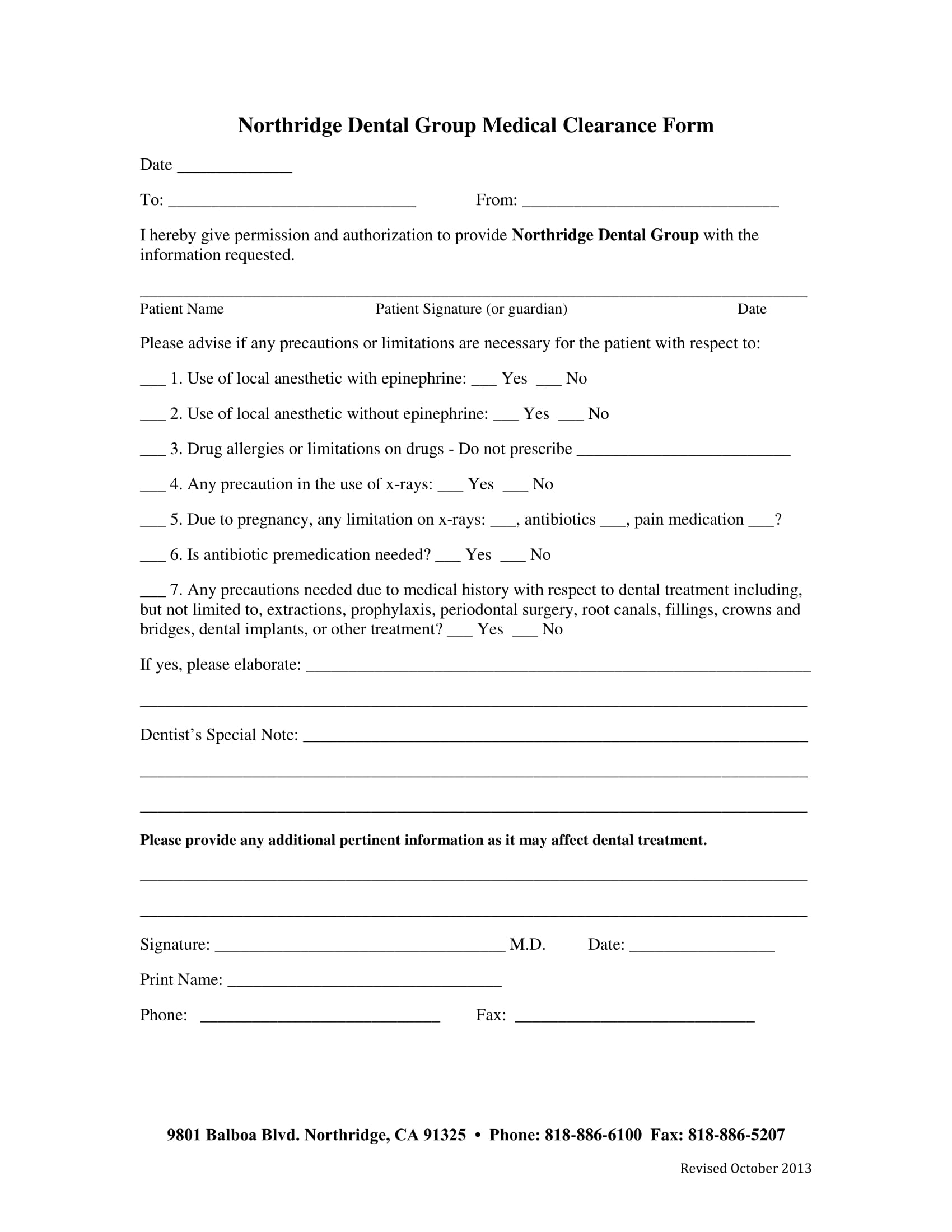
Medical Clearance For Dental Treatment Fill Online, Printable
Our mutual patient has presented for dental treatment with the following medical problem(s): This form is essential for obtaining medical clearance prior to dental treatment. Our mutual patient is scheduled for dental treatment. Medical clearance for dental treatment form. We appreciate your assistance in providing optimum care for this patient.
Printable Medical Clearance Form For Dental Treatment Printable Word
This form is essential for obtaining medical clearance prior to dental treatment. Medical clearance for dental treatment date: Our mutual patient has presented for dental treatment with the following medical problem(s): The following treatment is scheduled in our. This document is essential for obtaining medical clearance prior to dental procedures.

Printable Dental Clearance Form Printable Word Searches
This document is essential for obtaining medical clearance prior to dental procedures. This form is essential for obtaining medical clearance prior to dental treatment. Our mutual patient has presented for dental treatment with the following medical problem(s): The following treatment is scheduled in our. Our mutual patient, as noted above, is scheduled for.
Dental Medical Clearance Form Printable Printable Word Searches
Our mutual patient is scheduled for dental treatment. Medical clearance for dental treatment date: This form is essential for obtaining medical clearance prior to dental treatment. This document is essential for obtaining medical clearance prior to dental procedures. It ensures that the patient's medical history is reviewed by a.

Printable Medical Clearance Form For Dental Printable Forms Free Online
In an attempt to provide the best and safest dental care for this patient, we are requesting medical consultation and authorization. This document is essential for obtaining medical clearance prior to dental procedures. Our mutual patient has presented for dental treatment with the following medical problem(s): We appreciate your assistance in providing optimum care for this patient. Medical clearance for.
Printable Medical Clearance Form For Dental Treatment
Medical clearance for dental treatment date: It ensures that the patient's medical history is reviewed by a. In an attempt to provide the best and safest dental care for this patient, we are requesting medical consultation and authorization. Our mutual patient, as noted above, is scheduled for. Medical clearance for dental treatment form.
Our Mutual Patient, As Noted Above, Is Scheduled For.
In an attempt to provide the best and safest dental care for this patient, we are requesting medical consultation and authorization. Medical clearance for dental treatment form. It ensures that the patient's medical history is reviewed by a. This form is essential for obtaining medical clearance prior to dental treatment.
Our Mutual Patient Is Scheduled For Dental Treatment.
Our mutual patient has presented for dental treatment with the following medical problem(s): The following treatment is scheduled in our. Medical clearance for dental treatment date: This document is essential for obtaining medical clearance prior to dental procedures.