San Bernardino Bounds Portal Provider Enrollment Form - • going to the following website:. A new live scan form in your packet so that you can submit a new fingerprint background check. All of the steps are listed and need to be completed. Providers are encouraged to pick up an existing provider bounds packet (ihss pa 401 ep). If you do not agree with these requirements, please do not. Create an account in the bounds online provider enrollment portal (bounds) by: Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language, gender, adress,. This system is to be accessed by authorized users for business purposes only. You will need to register and complete the i. After completing orientation, you will need to complete and submit the “ihss provider enrollment agreement” form.
If you do not agree with these requirements, please do not. Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language, gender, adress,. You will need to register and complete the i. Create an account in the bounds online provider enrollment portal (bounds) by: • going to the following website:. A new live scan form in your packet so that you can submit a new fingerprint background check. After completing orientation, you will need to complete and submit the “ihss provider enrollment agreement” form. This system is to be accessed by authorized users for business purposes only. All of the steps are listed and need to be completed. Providers are encouraged to pick up an existing provider bounds packet (ihss pa 401 ep).
This system is to be accessed by authorized users for business purposes only. A new live scan form in your packet so that you can submit a new fingerprint background check. Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language, gender, adress,. You will need to register and complete the i. All of the steps are listed and need to be completed. After completing orientation, you will need to complete and submit the “ihss provider enrollment agreement” form. Create an account in the bounds online provider enrollment portal (bounds) by: If you do not agree with these requirements, please do not. Providers are encouraged to pick up an existing provider bounds packet (ihss pa 401 ep). • going to the following website:.
Login
After completing orientation, you will need to complete and submit the “ihss provider enrollment agreement” form. A new live scan form in your packet so that you can submit a new fingerprint background check. You will need to register and complete the i. Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language, gender,.
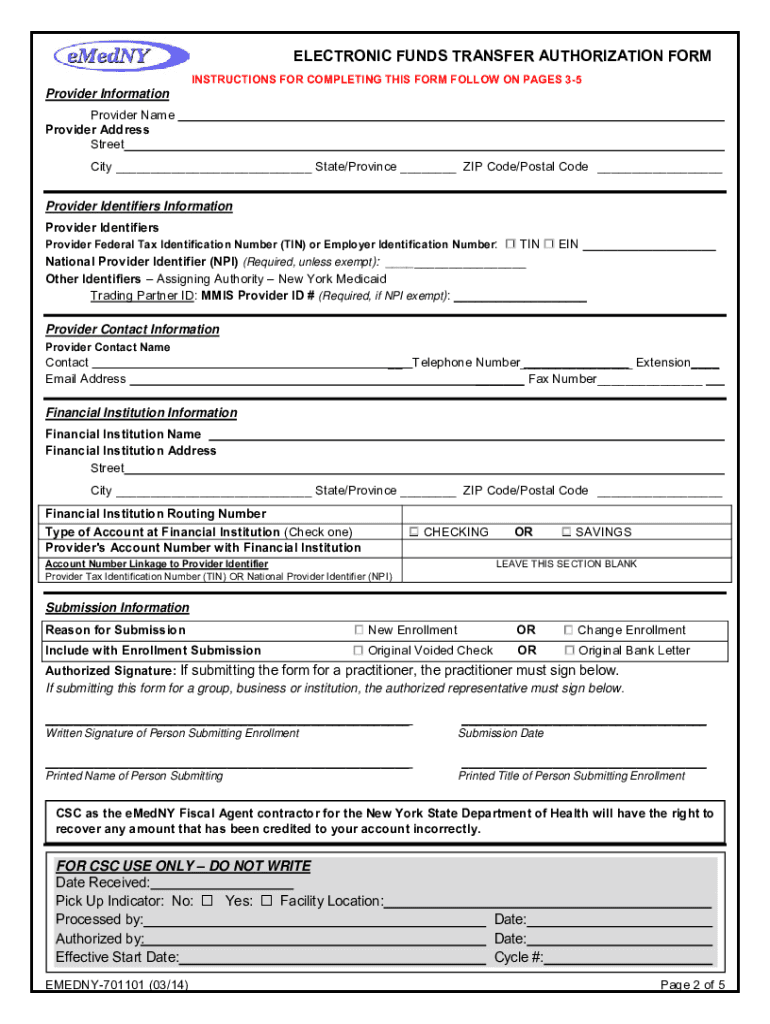
Emedny Eft Provider Enrollment Form Enrollment Form
All of the steps are listed and need to be completed. Providers are encouraged to pick up an existing provider bounds packet (ihss pa 401 ep). You will need to register and complete the i. Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language, gender, adress,. After completing orientation, you will need to.

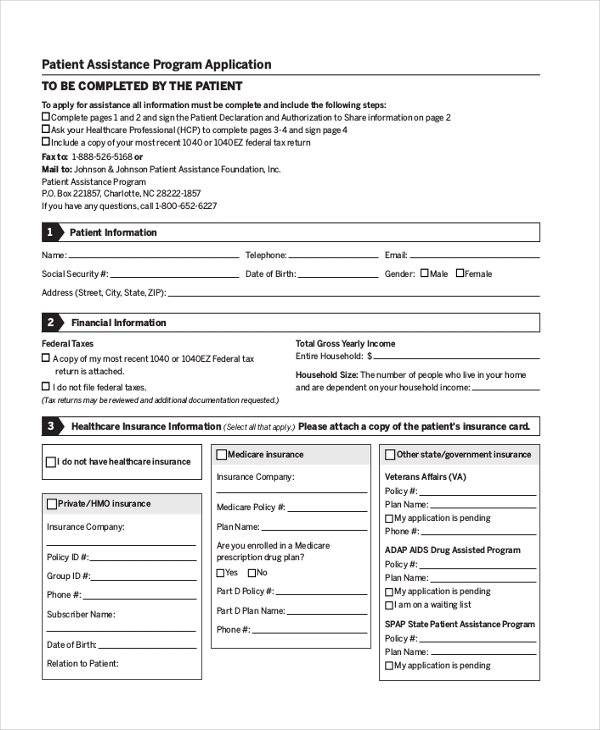
Texas Medicaid Provider Enrollment Application Form Enrollment Form
Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language, gender, adress,. Create an account in the bounds online provider enrollment portal (bounds) by: A new live scan form in your packet so that you can submit a new fingerprint background check. All of the steps are listed and need to be completed. After.
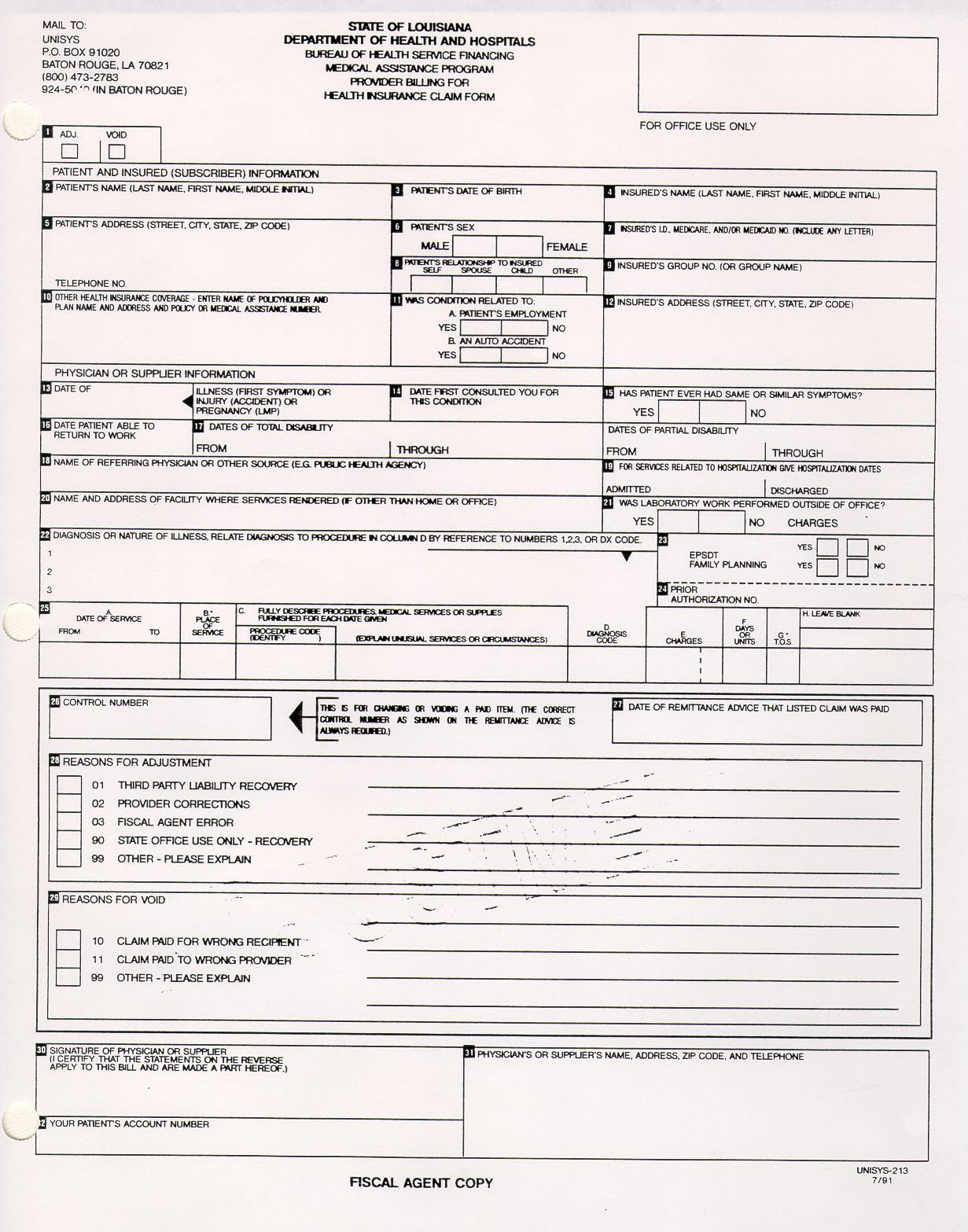
Mississippi Medicaid Provider Enrollment Form Enrollment Form
Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language, gender, adress,. A new live scan form in your packet so that you can submit a new fingerprint background check. You will need to register and complete the i. All of the steps are listed and need to be completed. This system is to.

Aetna Medicaid Provider Enrollment Form Enrollment Form
You will need to register and complete the i. Providers are encouraged to pick up an existing provider bounds packet (ihss pa 401 ep). If you do not agree with these requirements, please do not. After completing orientation, you will need to complete and submit the “ihss provider enrollment agreement” form. Create an account in the bounds online provider enrollment.

Fillable Online San bernardino bounds portal provider enrollment form
All of the steps are listed and need to be completed. Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language, gender, adress,. This system is to be accessed by authorized users for business purposes only. A new live scan form in your packet so that you can submit a new fingerprint background check..
Colorado Medicaid Provider Enrollment Update Form Enrollment Form
All of the steps are listed and need to be completed. Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language, gender, adress,. A new live scan form in your packet so that you can submit a new fingerprint background check. You will need to register and complete the i. Providers are encouraged to.
Ihss Provider Enrollment Form Enrollment Form
A new live scan form in your packet so that you can submit a new fingerprint background check. • going to the following website:. You will need to register and complete the i. All of the steps are listed and need to be completed. Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language,.
Ihss Provider Enrollment Form Soc 846 Enrollment Form
• going to the following website:. If you do not agree with these requirements, please do not. A new live scan form in your packet so that you can submit a new fingerprint background check. All of the steps are listed and need to be completed. Provider enrollment form please complete all fields below (ssn, dob, first & last name,.
Michigan Medicaid Provider Enrollment Form Enrollment Form
If you do not agree with these requirements, please do not. All of the steps are listed and need to be completed. You will need to register and complete the i. • going to the following website:. Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language, gender, adress,.
After Completing Orientation, You Will Need To Complete And Submit The “Ihss Provider Enrollment Agreement” Form.
A new live scan form in your packet so that you can submit a new fingerprint background check. This system is to be accessed by authorized users for business purposes only. Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language, gender, adress,. If you do not agree with these requirements, please do not.
Providers Are Encouraged To Pick Up An Existing Provider Bounds Packet (Ihss Pa 401 Ep).
All of the steps are listed and need to be completed. Create an account in the bounds online provider enrollment portal (bounds) by: You will need to register and complete the i. • going to the following website:.